The causes of azoospermia can be very different from one man to another, so a “no sperm” result should not immediately be assumed to mean the same thing for everyone. In clinical practice, doctors usually divide these causes into pre-testicular, testicular, and post-testicular groups, because each group carries different diagnostic and therapeutic consequences.
For couples waiting for a child, understanding the causes of azoospermia often helps reduce panic. Once the cause becomes clear, the conversation shifts from “is there still hope?” to “which step is the most appropriate for us to take?”.
Causes of azoospermia due to reproductive tract blockages
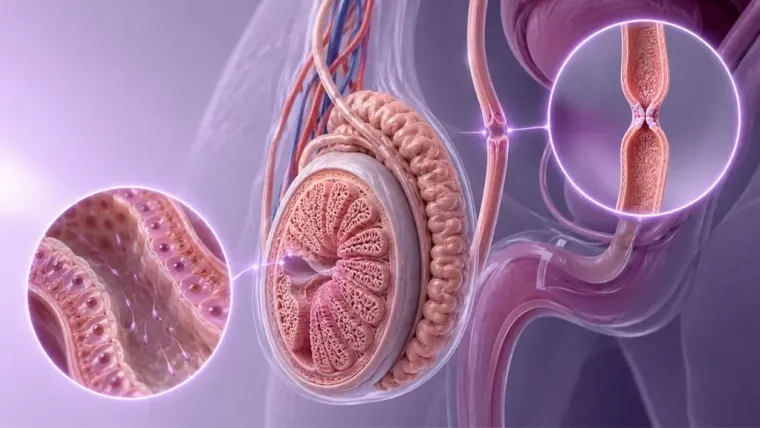
The first cause of azoospermia is obstruction, meaning sperm can still be produced but cannot exit with the ejaculate fluid. This blockage can be located in the epididymis (the small tube behind the testicles where sperm is stored and matured before exiting), the vas deferens (the tube that carries sperm from the testicles to the urethra — the tube that carries urine and ejaculate fluid out of the body through the penis), or the ejaculatory duct, including congenital conditions such as CBAVD (Congenital Bilateral Absence of the Vas Deferens — a condition where the vas deferens fails to form from birth on both sides).
In this group, low semen volume, acidic semen pH, or an impalpable vas deferens can be important clues. The American Urological Association (AUA) alongside the American Society for Reproductive Medicine (ASRM) and the European Association of Urology (EAU) all associate these findings with the possibility of obstruction, particularly in patients with suspected CBAVD or ejaculatory duct obstruction (a blockage in the ejaculatory duct — the duct connecting the vas deferens to the urethra).
Importantly, an obstruction does not automatically mean that sperm production is always damaged. Therefore, in certain cases, sperm retrieval or reconstruction can be considered.
Causes of azoospermia due to impaired sperm production in the testicles
The cause of azoospermia can also lie within the testicles themselves, namely when the process of sperm formation (spermatogenesis) experiences severe disruption. This is usually called NOA (Non-Obstructive Azoospermia — non-obstructive azoospermia, where the testicles do not produce sperm normally), and it can be related to primary testicular failure, a history of undescended testicles (cryptorchidism), exposure to substances harmful to the testicles such as chemotherapy or radiation (gonadotoxins), or certain genetic abnormalities.
Klinefelter syndrome is one of the most frequently discussed genetic causes in this context. The EAU notes this condition as the most common sex chromosome abnormality — where a man has an extra X chromosome (47,XXY), and although many patients experience severe sperm production impairment, sperm retrieval is still possible in some appropriately selected cases.
Y-chromosome microdeletions are also relevant. The 2024 AUA/ASRM guideline update estimates this abnormality is present in about 8–12% of men with NOA, making genetic evaluation essential before discussing next steps.
Causes of azoospermia due to hormonal disorders or pre-testicular factors
Some causes of azoospermia originate from hormonal disorders, particularly when the hypothalamic–pituitary–testicular axis (the hormonal system connecting the brain and testicles to regulate sperm production) is not working properly. In the condition of hypogonadotropic hypogonadism (HH) — a condition where the brain does not send enough hormonal signals to the testicles, impairing sperm production, hormonal stimulation to the testicles is low causing spermatogenesis to be disrupted, but in some patients, this is actually the group most likely to improve with the right therapy.
Certain medications can also be a factor. The AUA/ASRM asserts that testosterone monotherapy must not be given to men who still desire fertility, because its negative feedback can suppress gonadotropins (hormones from the brain that stimulate the testicles to produce sperm) and even cause azoospermia.
Environmental and behavioral factors are not always the sole causes, but they can worsen male reproductive health. ESHRE (European Society of Human Reproduction and Embryology — the European reproductive and embryology organization) places impaired sperm quality and function, hormonal factors, injuries, infections, and congenital abnormalities of the genital tract as part of the spectrum of causes of male infertility.
Why knowing the cause of azoospermia changes treatment choices
Knowing the cause of azoospermia makes therapy choices much more rational. If the source of the problem is an obstruction, the couple can discuss sperm retrieval or reconstruction; if the main source is hormonal, hormonal therapy can be an important part; if the problem is NOA, the focus often shifts to the possibility of sperm retrieval via micro-TESE and IVF & ICSI programs.
On the other hand, genetic evaluation results can also change decisions. In certain examples such as the complete deletion of the AZFa or AZFb regions on the Y chromosome (complete AZFa or AZFb microdeletions) — a genetic condition where the genes responsible for sperm production are completely missing — the EAU states the chance of sperm retrieval is zero, so surgery is not recommended. Information like this is indeed heavy, but it actually helps couples avoid unnecessary procedures.
Understanding the causes of azoospermia is not merely a list of risk factors — what is more important is how those causes lead to different therapeutic decisions for every couple.
Conclusion
The causes of azoospermia can originate from tract blockages, impaired sperm production in the testicles, or pre-testicular hormonal disorders. Each brings different consequences to follow-up testing, sperm retrieval chances, and family planning options.
The faster the cause of azoospermia is accurately identified, the smaller the risk of couples wasting time on less relevant steps. This is important not only for therapy efficiency, but also for keeping hope grounded in accurate information.
Next Steps
If your results already point to azoospermia, the most useful next step is ensuring whether the problem tends to be a blockage, hormonal, or a sperm production disorder.
Free HagiaMed Consultation — a free initial consultation with our specialists, with no cost and no commitment.
References
• American Urological Association and American Society for Reproductive Medicine. Diagnosis and Treatment of Infertility in Men.
• European Association of Urology. Sexual and Reproductive Health Guidelines: Male Infertility.
• Flannigan R, et al. 2023 Canadian Urological Association guideline: Evaluation and management of azoospermia.
Disclaimer: This information is educational in nature and does not replace a doctor’s evaluation. Diagnostic and therapeutic decisions must be tailored to the examination results of you and your partner.



